Tuberculosis if tested early can prevent the spreading of the disease. Also the treatment methods now are such that it helps in understanding the characteristic of the M.tuberculosis thus it helps in drug administration. Testing for Latent TB Tuberculosis skin test (or PPD) It is mostly used to test Latent TB(see Signs and Symptoms). The World Health Organization estimates that 2 billion people worldwide have latent TB, while around 3 million people worldwide die of TB each year. The Tuberculosis Skin Test is also called as Tuberculin test or PPD ( Purified Protein Derivative) Recommended for people who-
 After 48-72 hours the doctor or nurse will check if there is any reaction to it. If the result is negative then it means that the individual has no TB infection. By negative infection it means that the skin where the shot has been given is not swollen and or the swelling is very small. This measurement is different for children, people with HIV, and other high risk groups. If the results are positive then it means that the individual has TB infection and that treatment is required. By positive results it means that there will be redness, swelling.  Image url : http://upload.wikimedia.org/wikipedia/commons/9/9d/Mantoux_test.jpg The tuberculin skin test is based on the fact that infection with M.tuberculosis bacterium produces a delayed-type hypersensitivity skin reaction to certain components of the bacterium[1]. The components of the organism are contained in extracts of culture filtrates and are the core elements of the classic tuberculin PPD (also known as purified protein derivative) [1]. This PPD material is used for skin testing for tuberculosis[1]. Reaction in the skin to tuberculin PPD begins when specialized immune cells, called T cells, which have been sensitized by prior infection, are recruited by the immune system to the skin site where they release chemical messengers called lymphokines[1]. These lymphokines induce induration (a hard, raised area with clearly defined margins at and around the injection site) through local vasodilation (expansion of the diameter of blood vessels) leading to fluid deposition known as edema, fibrin deposition, and recruitment of other types of inflammatory cells to the area[1]. This measurement is different for children, people with HIV, and other high risk groups[2]. This is not a perfect test[2]. Up to 1 in 5 people infected with the bacteria that cause TB may not have a reaction[2]. Also, diseases or medicines that weaken the immune system may cause a false-negative result[2]. Also in many countries BCG vaccine is given. This vaccine may produce false positve test[2]. However, most experts say that a past BCG vaccination should not change the PPD result when the test is done in people with an increased risk of TB infection or disease[2]. Interferon γ Release Assays (IGRAs): There are two approved methods of this test[3]
To conduct the tests fresh blood samples are mixed with antigens and controls. The antigens, testing methods and interpretation criteria for IGRAs differ ( see the table given below)
Table: http://www.cdc.gov/tb/publications/factsheets/testing/igra.htm ADVANTAGES
Testing for Active TB Diagnosing active Tuberculosis based merely on signs and symptoms is difficult, as is diagnosing the disease in those who are immunosuppressed[4]. A diagnosis of TB should, however, be considered in those with signs of lung disease or constitutional symptom lasting more than two weeks[4]. Radiological symptom- CT scan and Chest X-Ray: Chest X-rays are used to detect any abnormalities in lungs. 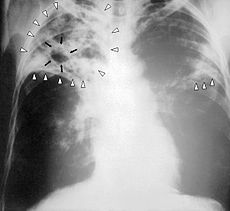 The chest x-ray has poor sensitivity as in the early stages of disease, the damage to the lungs may not yet have become sufficiently marked to be detectable so people who have active TB are missed. Even experienced radiologists have difficulty in detecting abnormality. Therefore the results from a chest x-ray cannot confirm that a person has TB disease. In the 40% of all cases of active TB where the disease is not found in the lungs (extra or non-pulmonary TB) the chest x-ray is of no use. In some hospitals Computerised Tomography (CT Scan) and Magnetic Resonance Imaging (MRI) have proved useful for imaging tuberculosis lesions, particularly those in the brain and spine[5]. CT scans are therefore often used to identify non-pulmonary TB[5]. AFB staining Sputum of the individual is taken and is tested for the presence of M.tuberculosis by staining it. Stains specific for staining of acid fast bacteria is used here. Mostly Ziehl Neilson acid fast stain is used. 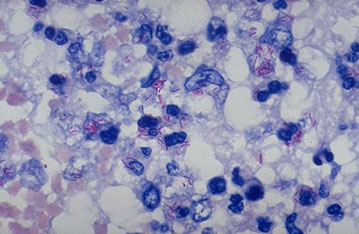 However, the WHO estimates that it only identifies 35% of patients with active TB[5]. As the test identifies cells suspended in liquid samples it has particular difficulty in detecting many forms of non-pulmonary TB which occur in a variety of organs in the body[5]. This test will also identify acid fast bacilli other than M. tuberculosis so its specificity is not 100%[5]. Despite these shortcomings it is still the front line tool for active TB diagnosis, partly because the more definitive culture techniques take longer and because it can also determine if a person is infectious[5]. Culture techniques Culture techniques are still seen as the gold standard for active TB as they are extremely sensitive, so long as live mycobacteria can be obtained in the sample[5]. M. tuberculosis can be cultured from a variety of specimens including sputum, Central Spinal Fluid (CSF), pleural effusion, bronchoalveolar lavage (BAL), gastric aspirate etc and can thus be used to detect pulmonary as well as non-pulmonary disease[5]. By assessing the effect of antibiotics on the cultured bacilli, this technique can also identify the antibiotic susceptibility of the particular strain of TB infecting the patient[5]. It is therefore the main method for identifying if a person has multi-drug resistant (MDR) TB[5]. However, it is not always possible to obtain mycobacteria in the sample, especially in non-pulmonary TB so culture is not a sensitive test[5]. If performed correctly it should have very high specificity and can distinguish M. tuberculosis from other mycobacteria[5]. A drawback of this test is the time to result which can be anything from 2 to 6 weeks[5].Treatment is often begun before cultures are confirmed[4].
NAAT Nucleic acid amplification tests (NAATs), such as polymerase chain reaction (PCR), are a relatively new development in active TB testing[5]. Even though NAAT techniques can magnify even the smallest amounts of genetic material, the sample used still has to contain a certain number of TB bacilli and this is not always possible, particularly with non-pulmonary TB where sensitivity can be as low as 60%[5]. More recently NAATs have been used to identify MDR TB as mutations in the DNA of MTB which confer drug resistance have been discovered. These methods are quicker than culture but generally only identify resistance to rifampicin and isoniazid[5]. References [1]MedicineNet.com n.d.,Tuberculosis skin test (PPD skin test), viewed 11 September 2012, http://www.medicinenet.com/tuberculosis_skin_test_ppd_skin_test/article.htm [2]MedlinePlusn.d, PPD skin test, viewed 11 September 2012, http://www.nlm.nih.gov/medlineplus/ency/article/003839.htm [3] CDC n.d.,Interferon-Gamma Release Assays (IGRAs) Blood test for TB infection, viewed 11 September 2012, [4]Wikipedia the free encyclopedia n.d.,Tuberculosis, viewed 11 September 2012, [5]Oxford Immunotech, Tuberculosis, viewed 11 September 2012, |
|||||||||||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}